


What is the Most Common Risk of Exposure to Bloodborne Pathogens for Healthcare Workers? Healthcare workers are always involved in providing patient care. They are defined as the population at risk of occupational exposure to pathogens are very large. The World Health Organisation reported that more than 3 million health care workers worldwide are exposed to some kind of bloodborne pathogens. Bloodborne pathogens, such as hepatitis A, B and C, can cause infectious disease. Healthcare workers are in contact with potentially infectious materials daily.
It is important to know the general risks to health workers of exposure to bloodborne pathogens in order to be able to work safely. In this detailed guide, we will focus on key risks to health of blood-borne pathogens, followed by the safety precautions to prevent it. So let’s get started!
Table of Contents
What is the most common occupational risk for blood-borne pathogen exposure (USA)?
The occupational hazards faced by US health care workers every day are very numerous. Bloodborne Pathogens are among the most significant occupational hazard. Short answer: The most common manner of exposure and thus the most significant source of occupational bloodborne pathogen transmission.
This is an in-depth explanation that details what the most common risk is, which pathogens are most dangerous, statistics involving transmission, OSHA-mandated prevention techniques, and post-exposure procedures that all healthcare personnel should be familiar with.
Search Intent & User Needs Analysis
Dominant search intent: Informational User’s problem:
Healthcare workers, students, and safety officers are looking to pinpoint the greatest risk for exposure to bloodborne pathogens to enhance prevention efforts and response protocols after an exposure.
Users’ needs:
- Identification of the #1 risk
- HBV, HCV, and HIV transmission rates
- OSHA requirements and related precautions
- Post-exposure treatment and timeline
- Actionable safety protocol recommendations
The Most Common Risk: Percutaneous (Sharps) Injuries
Why Needlestick Injuries Dominate Exposure Statistics
Percutaneous injuries, punctures through the skin by needles, scalpels, lancets, and other sharps, are the most common mode of transmission of bloodborne pathogens in healthcare.
Key statistics:
| Metric | Statistic | Source |
| Hospitals in the US are trying to get the inclusion of one year’s worth of sharps injury data. | ~385,000 | |
| Daily sharps injuries (hospitals) | 1,000+ | |
| Number of Injuries per year (all settings) | 600,000–800,000 | |
| Highest-risk occupation | Nurses | |
| Most common injury cause | Disposing of used needles (39.83%) |
Sharps injuries: 1.93 per 100 HCWs/year to mucocutaneous exposure (Eye 0.11 per 100/yr, skin 0.04 per 100/yr).
Top 3 Bloodborne Pathogens of Concern
More than twenty blood-borne pathogens exist; three viruses make up the most common occupational infections:
Transmission Risk Comparison
| Pathogen | Transmission Risk After Percutaneous Exposure | Key Facts |
| Hepatitis B (HBV) | 6–30% (if unvaccinated) | -Infectious’ can remain infectious for 1 week on surfaces. |
| Hepatitis C (HCV) | 1.8% | Most common blood-borne infection in US. No vaccine. |
| HIV | 0.3% (1 in 300) | Lowest risk (no need for PEP if condom used), PEP is effective if given within 72 hrs |
Key differences: HIV received the most media coverage, HBV is the most likely to infect an individual (up to 100x more so than HIV), and HCV is the most common chronic blood-borne infection in the US.
Who Should Be Concerned?
High-Risk Departments & Occupations
The practitioners most at risk of exposure are those who perform repetitive invasive procedures and are exposed to high volumes of blood or those working in acute care.
| Department/Risk Level | ‘Incidence Rate’ (per 100 workers) |
| Dental Clinic | 9.83 |
| Department of Surgery | 2.86 |
| Department of Internal Medicine | 2.25 |
| Overall Average | 2.22 |
Occupation breakdown:
- Nurses aides: 5.79 per 100 (second highest)
- Doctors: 2.28 per 100
- Nurses: 1.69 per 100
Accordingly, the majority of needlestick injuries were found among nurses, mostly in the patient wards, operating theatre and RECOVERY.
How Bloodborne Pathogens Transmit
Primary Transmission Routes
1. Percutaneous injury (needlestick) Most common
2. Mucocutaneous exposure (splashes to eyes, nose..)
3. Cuts, abrasions, or bites contacting infected fluids
4. Contact with visibly blood-contaminated fluids
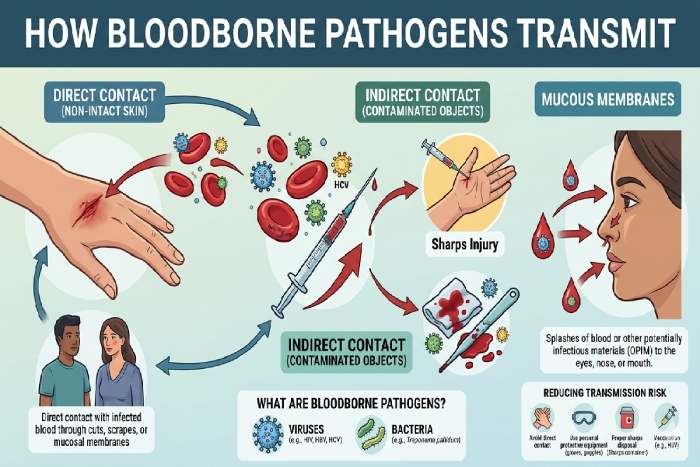
Potentially Infectious Materials (OPIM)
Not just blood these substances also transmit pathogens:
- Blood
- Semen and vaginl secretions
- 7.22 Cerebrospinal, synovial, pleural, pericardial and amniotic. These can be sent for fungus culture and microscopy.
- Engl5005/20 Contimplated blood causes the secretion of saliva and urine.
OSHA Bloodborne Pathogens Standard: Mandatory Protections
The protection from bloodborne pathogens standard has been in place since 1991.
Employer Requirements
| Requirement | Detail |
| Exposure Control Plan | Filed yearly. 5» focuses on the task of possible casualties and manpower available for the task. |
| Hepatitis B Vaccine | Published 10 days or less before the assignment |
| Training | Initial+annual; interactive Q and A required |
| Engineering Controls | Sharps containers, safety-engineered devices |
| PPE Provision | Gloves, gowns, face shields, eye protectiv |
| Sharps injury log required. | employee confidentiality maintained |
| After Exposure, follow up with | Immediate medical assessment + testing |
Hierarchy of Controls (Most Effective to Least Effective)
1. Elimination/Substitution -needleless systems, blunted suture needles
2. Engineering controls – sliding sharps, retractable needles
3. Operational controls– do not recap, dispose of, and use the biohazard label
4. PPE- gloves, mask, eye shield, apron
Common causes of needlestick injuries

CDC analysis reveals the top injury scenarios:
| Cause | Percentage |
| Manipulating the needle in the patient | 27% |
| Improper disposal/disposal-related | 22% |
| Cleanup | 11% |
| Handling/passing the device during/after use | 10% |
Nearly all needlestick exposures are due to the disposal of sharps. This demonstrates that sharps should always be disposed of in lidded sharps containers. Take care not to overfill them.
Post-Exposure Prophylaxis (PEP): What to do following exposure
Immediate first-aid measures
- Neddlesh/cuts: Zmackej with soap (diluted water)
- Nose/mouth splashes: rinse with water
- Eye: Flush with water, sterile irrigants (10.12.1) or saline
- Report immediately to the supervisor
PEP Timeline by Pathogen
| Pathogen | PEP Recommended? | Critical Timeline |
| HBV | Yes | The maximum is not to be more than 24 hours in 24 hours(max 24hours). Please provide the time, which should preferably not be even or more than 24 hours during the process. |
| HCV | No | Just supervisor; no PEPs available |
| HIV | Yes | Within hours (must start within 72hours): |
Follow-Up Testing Schedule
| Pathogen | Testing Timeline |
| HBV | Anti-HB test 1-2 months after last dose (if vaccine only administered) |
| HCV | Other methods of early diagnosis: Anti-HCV + ALT at 4-6 months, and HCV RNA at 4-6 weeks |
| HIV | Basal line +6weeks, 3 months, 6 months. Check for drug toxicity after 2 weeks. |
Emergency Contact: Clinicians’ Post Exposure Prophylaxis Line: 1-888-448-4911
Prevention Strategies That Work
Safety-Engineered Devices Reduce Injuries
Sharps injuries in nonsurgical hospital units declined 31.6% since the Needlestick Safety and Prevention Act (2000), (2001–2006).
- Devices with sharps injury protection (SIP) include:
- Retracting needles
- Sliding sheaths
- Hinged needle shields
- Needleless systems
Best Practices for Healthcare Workers
Do:
- Use safety-engineered devices consistently
- Activate safety features immediately after use
- Place sharps in puncture-resistant, labelled containers.
- Monitory container filling levels (never overspill)
- Wash hands
- Before wearing and
- After removing PPE
- HBV vaccination if not immune
Don’t:
- Recap needles (unless no alternative exists)
- Place non-sharps in sharps containers
- Work in overcrowded procedure areas
- Ignore exposure reporting protocols
- Skip PPE even for “low-risk” procedures
Common Mistakes & Misconceptions
Critical Errors Healthcare Workers Make
| Mistake | Why It’s Dangerous |
| Underreporting exposures | ~50% of sharps injuries go unreported; delays PEP |
| Assuming low-risk exposure | Unknown patient status = treat as infectious |
| Skipping HBV vaccination | 6–30% transmission risk if unvaccinated |
| Improper PPE fit | Loose gowns/gloves reduce protection significantly |
| Recapping needles | The major cause of preventable needlesticks |
Myth: “HIV is the biggest risk”
Reality: HIV transmission risk (0.3%) is 20× lower than HCV (1.8%) and 60–100× lower than HBV (6–30%). Hepatitis viruses pose a far greater occupational threat.
FAQ Section
The most transmissible blood-borne pathogen is.
Hepatitis B (HBV) has the highest risk of transmission (6 30%) postpercutaneous exposure when compared to other blood-borne pathogens.
Is there a post-exposure prophylaxis for hepatitis C
No. PEP should not be used for HCV. You only have testing and monitoring.
How soon after the exposure can HIV PEP be initiated?
HIV PEP should be started within hours of exposure to be effective, and must be taken within 72 hours.
Which healthcare workers are most affected by needlestick injuries?
Nurses and nurse‘s aides tend to sustain the most needlestick injuries with the highest number of injuries sustained in the general wards and operating theatres.
Can Hepatitis B last on dry surfaces?
HBV can live outside the human body and remains infectious on environmental surfaces for as long as seven days.
Final Conclusion
Understanding the hazards of the routine bloodborne pathogen exposures faced by health care workers is a key element to making a workplace safer. One has to be committed to agreeing to enrol for the training, using the procedure, and having a safety consciousness. Through faith in continued education and diligence, everyone wins to create a safer and healthier workplace.