


Spinal Surgery Indications Risks and Recovery. Spinal surgery is a huge medical choice that can have a significant effect on the quality of your life. Although never before have the methods of surgery made the spine operations a safer and more effective process than before, it is crucial to know when it is necessary to have an operation, what the risk may be, and what the recovery process will entail to make a well-informed decision.
This is an informative book that will give you all the information on the subject of spinal surgery indications, complications, and the process of recovery.
Table of Contents
A basic guide to Spinal Surgery: What you should know.
Spinal surgery is a set of processes aimed at eliminating pain, restoring the functions, and avoiding additional spinal cord and spine damage. The operations are used to treat structural issues that squeeze nerves, destabilize the spine, or result in permanent debilitating pain.
When Non-Surgery is not Sufficing.
Surgery is normally an option of last resort when non-surgical methods of treatment are found to be inadequate in terms of relief. In the majority of cases of back and neck pain a non-surgical strategy within 6-12 weeks results in the relief of the pain and includes:
- Physical therapy
- Medications (NSAIDs, muscle relaxants, pain relievers)
- Epidural steroid injections
- Chiropractic care
- Lifestyle modifications
Surgery becomes appropriate when:
- Pain continues to exist 6-12 months after the use of aggressive conservative therapy.
- There are progressive degenerations of the nervous system (weakness, numbness, bowel/bladder loss)
- The quality of life is extremely impaired.
- Morphological instability poses a risk to the spinal cord.
Important: Many imaging findings like disc bulges or arthritis are normal age-related changes and don’t automatically require surgery.
How Spine Surgery Works
Spinal surgery achieves pain relief and functional improvement through several mechanisms:
- Decompression – Removing pressure on pinched nerves or the spinal cord
- Stabilization – Fusing unstable vertebrae to prevent abnormal motion
- Restoration – Correcting alignment or replacing damaged disc material
- Prevention – Stopping progressive deformity or neurological deterioration
Minimally invasive procedures involving small incisions, special instruments and sophisticated imaging guidance are becoming more popular as a trend in modern practice.
Who Performs Spinal Surgery
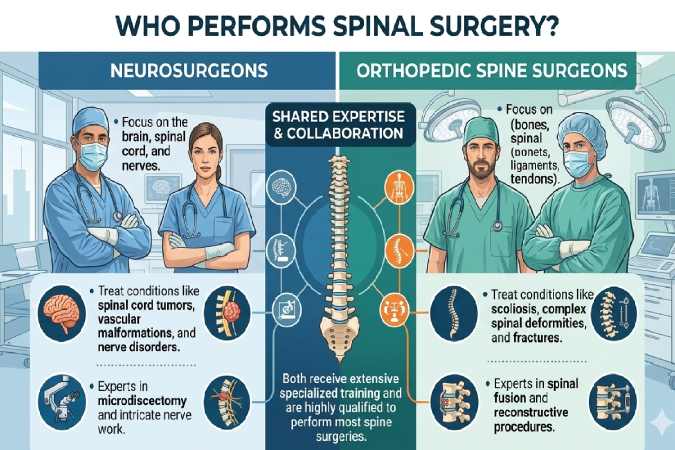
Spinal surgery is performed by:
- Orthopedic spine surgeons – Specialize in musculoskeletal spine conditions
- Neurosurgeons – Focus on nervous system and spinal cord pathology
Both are qualified, though individual expertise varies. Choose a surgeon who:
- Performs high volumes of your specific procedure
- Is board-certified in their specialty
- Works at a comprehensive spine center
- Communicates clearly and answers all questions
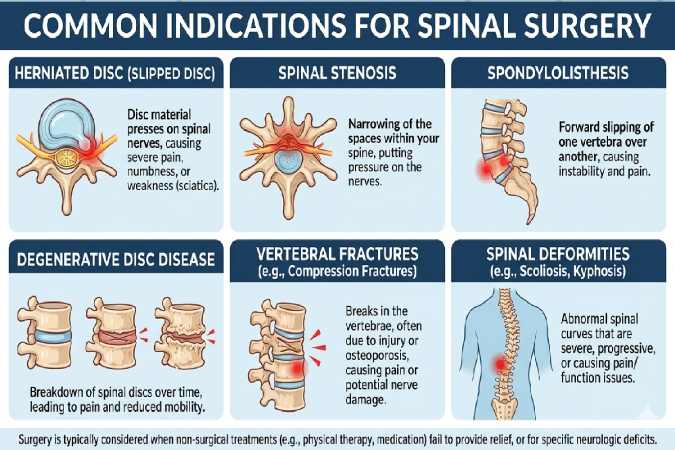
Indications for Spinal Surgery: When Is It Necessary?
Spinal Surgery Indications Risks and Recovery. Understanding the specific conditions that may require surgical intervention helps determine if you’re a candidate.
Herniated or Bulging Discs
What it is: The gel-like center of an intervertebral disc pushes through its outer layer, compressing nearby nerves.
Symptoms:
- Sharp, shooting pain down the leg (sciatica) or arm
- Numbness or tingling
- Muscle weakness
- Pain worsens with sitting, bending, or coughing
Surgical indication:
- Severe symptoms lasting >6-12 weeks
- Progressive weakness
- Cauda equina syndrome (emergency – loss of bowel/bladder control)
Typical surgery: Discectomy or microdiscectomy
Spinal Stenosis
What it is: Narrowing of the spinal canal that squeezes the spinal cord or nerve roots.
Symptoms:
- Leg pain with walking (neurogenic claudication)
- Relief when bending forward or sitting
- Numbness, tingling, or weakness in legs
- Balance problems
Surgical indication:
- Inability to walk acceptable distances
- Significant impact on daily activities
- Conservative treatment failure after 3-6 months
Typical surgery: Laminectomy with or without fusion
Degenerative Disc Disease
What it is: Wear-and-tear breakdown of intervertebral discs causing pain and instability.
Symptoms:
- Chronic low back or neck pain
- Pain increases with activity
- Stiffness, especially in morning
- Occasional radiating pain
Surgical indication:
- Disabling pain unresponsive to extensive conservative care
- Documented disc collapse with instability
- Note: This diagnosis alone rarely requires surgery
Typical surgery: Spinal fusion or disc replacement
Spondylolisthesis
What it is: One vertebra slips forward over the one below it.
Symptoms:
- Low back pain
- Leg pain or numbness
- Tight hamstrings
- Changes in posture or gait
Surgical indication:
- Progressive slippage (>50%)
- Neurological symptoms
- Unstable spine
- High-grade slips in adolescents
Typical surgery: Decompression with fusion
Spinal Fractures and Trauma
What it is: Broken vertebrae from accidents, falls, or osteoporosis.
Surgical indication:
- Unstable fractures
- Neurological compromise
- Progressive deformity
- Severe pain not controlled with bracing
Typical surgery: Vertebroplasty, kyphoplasty, or instrumented fusion
Spinal Tumors or Infections
Surgical indication:
- Neurological compromise
- Structural instability
- Biopsy needed for diagnosis
- Failed medical management of infection
Typical surgery: Tumor resection, debridement, reconstruction
Scoliosis and Spinal Deformities
Surgical indication:
- Curves >50 degrees (especially in growing children)
- Progressive deformity
- Pain and functional impairment
- Cardiopulmonary compromise
Typical surgery: Corrective fusion with instrumentation
When Surgery May NOT Be Indicated
Red flags suggesting surgery may not help:
- Diffuse, non-specific pain without clear anatomical cause
- Pain as only symptom (no neurological findings)
- Psychological factors (severe depression, catastrophizing)
- Active litigation or compensation claims
- Multiple prior failed surgeries
- Smoking (significantly reduces fusion success)
- Unrealistic expectations
Types of Spinal Surgery Procedures
Different spinal conditions require different surgical approaches. Here’s what each procedure involves:
Spinal Fusion
Purpose: Permanently join two or more vertebrae to eliminate painful motion.
How it works:
- Bone graft placed between vertebrae
- Metal rods and screws hold bones in position
- Over 3-12 months, bones grow together (fuse)
Indications: Instability, spondylolisthesis, degenerative disc disease, scoliosis
Recovery time: 3-6 months for fusion, up to 12 months full recovery
Success rate: 70-90% pain improvement
Considerations:
- Limits spinal flexibility
- Adjacent segment degeneration risk (10-15% over 10 years)
- Non-fusion (pseudoarthrosis) occurs in 5-10%
Laminectomy
Purpose: Remove part of the vertebral bone (lamina) to relieve pressure on spinal cord or nerves.
How it works:
- Surgeon removes the lamina and any bone spurs or thickened ligaments
- Creates more space for nerves
- May be combined with fusion if spine becomes unstable
Indications: Spinal stenosis, herniated discs, tumors
Recovery time: 6-12 weeks
Success rate: 80-90% for leg pain relief
Considerations:
- May cause spinal instability requiring fusion
- Symptom recurrence possible over time
Discectomy/Microdiscectomy
Purpose: Remove herniated disc material pressing on a nerve.
How it works:
- Small incision (microdiscectomy uses 1-1.5 inch incision)
- Operating microscope provides magnified view
- Portion of disc causing compression removed
- Remaining disc left intact
Indications: Herniated disc with radiculopathy (nerve pain)
Recovery time: 4-6 weeks
Success rate: 85-95% for leg/arm pain relief
Considerations:
- 5-15% re-herniation rate
- Usually does not eliminate back/neck pain entirely
- Minimally invasive technique allows faster recovery
Foraminotomy
Purpose: Enlarge the neural foramen (opening where nerve roots exit) to relieve compression.
How it works:
- Remove bone and tissue around nerve opening
- Decompresses pinched nerve
- Can be done minimally invasively
Indications: Foraminal stenosis, bone spurs compressing nerve
Recovery time: 4-8 weeks
Success rate: 75-90%
Artificial Disc Replacement
Purpose: Replace damaged disc with artificial implant while preserving motion.
How it works:
- Damaged disc removed from front (anterior approach)
- Artificial disc (metal and plastic components) inserted
- Allows continued spine flexibility
Indications: Single-level degenerative disc disease, younger patients
Recovery time: 6-12 weeks
Success rate: Similar to fusion but preserves motion
Considerations:
- Only approved for certain spine levels
- Long-term durability still being studied
- Not suitable if arthritis or instability present
Minimally Invasive Spine Surgery
Modern techniques allow many procedures through smaller incisions using:
- Tubular retractors
- Endoscopic cameras
- Image guidance systems
Advantages:
- Less muscle damage
- Reduced blood loss
- Faster recovery
- Shorter hospital stay
- Less post-operative pain
Not appropriate for:
- Complex deformities
- Multi-level fusions
- Revision surgeries
- Certain anatomical challenges
Choosing the Right Procedure
The best surgery depends on:
- Your specific diagnosis
- Location (cervical, thoracic, lumbar)
- Number of levels involved
- Your age and health status
- Activity goals
- Surgeon expertise
Always ask: “What would you recommend if I were your family member?”
Risks and Complications of Spinal Surgery
While modern spine surgery is generally safe, all procedures carry risks. Understanding these helps you make informed decisions and recognize problems early.
Common Risks (Occurring in 1-5% of Cases)
Infection
- Superficial wound infections: 1-3%
- Deep infections requiring additional surgery: <1%
- Higher risk with: diabetes, obesity, smoking, prolonged surgery
Prevention:
- Prophylactic antibiotics
- Sterile technique
- Glucose control in diabetics
Bleeding
- Excessive blood loss requiring transfusion: 1-5%
- Hematoma formation: rare but can compress nerves
Blood Clots (DVT/PE)
- Deep vein thrombosis: 1-3%
- Pulmonary embolism: <1%
Prevention:
- Early mobilization
- Compression stockings
- Blood thinners in high-risk patients
Dural Tear (Spinal Fluid Leak)
- Occurs in 1-3% of surgeries
- Usually repaired during surgery
- May cause headaches if unrecognized
- Generally heals well with bedrest
Serious Neurological Complications
Nerve Root Injury
- Occurs in <1% of cases
- Can cause new weakness, numbness, or pain
- May be temporary or permanent
- Risk higher in revision surgeries
Spinal Cord Injury
- Extremely rare (<0.1%)
- Can cause paralysis or severe disability
- Risk higher in cervical and thoracic surgery
- Monitoring during surgery reduces risk
Cauda Equina Syndrome
- Emergency complication
- Loss of bowel/bladder control
- Severe leg weakness
- Saddle numbness
- Requires immediate surgical decompression
Failed Back Surgery Syndrome
Persistent or worsening pain after spine surgery affects 10-40% of patients.
Causes:
- Wrong surgery or level operated
- Incomplete decompression
- Recurrent herniation
- Scar tissue (epidural fibrosis)
- Adjacent segment degeneration
- Nerve damage during surgery
- Unrealistic expectations
Prevention:
- Correct diagnosis before surgery
- Appropriate patient selection
- Skilled surgical technique
- Comprehensive rehabilitation
Hardware Complications
With instrumented fusions:
- Screw/rod loosening: 2-5%
- Hardware breakage: 1-2%
- Screw malposition: <1%
- Pseudoarthrosis (non-fusion): 5-10%
Risk factors:
- Smoking (triples non-fusion rate)
- Osteoporosis
- Multi-level fusion
- Obesity
Anesthesia Risks
General anesthesia carries risks including:
- Allergic reactions (rare)
- Breathing problems
- Heart complications
- Stroke (extremely rare)
- Death (<1 in 100,000)
Higher risk with:
- Advanced age
- Heart/lung disease
- Obesity
- Sleep apnea
Long-Term Complications
Adjacent Segment Disease
- Degeneration of levels next to fusion
- Occurs in 10-15% over 10 years
- May require additional surgery
Chronic Pain
- Some patients have ongoing pain despite “successful” surgery
- Related to nerve changes, scar tissue, muscle deconditioning
Loss of Flexibility
- Fusion procedures eliminate motion at treated levels
- Can impact activities requiring spinal flexibility
Risk Factors That Increase Complications
Patient factors:
- Smoking: Increases all complication rates 2-4x
- Diabetes: Higher infection risk
- Obesity: Increased wound complications, longer surgery
- Osteoporosis: Hardware failure risk
- Depression: Poorer outcomes
- Workers’ compensation: Lower satisfaction rates
Surgical factors:
- Revision surgery: 2-3x higher complication rates
- Multi-level procedures: Additive risks
- Combined approaches: More complex
- Surgeon experience: Lower volumes = higher complications
Spinal Surgery Recovery Timeline
Recovery is a gradual process with distinct phases. Understanding what to expect helps you plan appropriately and recognize complications early.
Hospital Stay: Days 1-4
Immediately After Surgery:
- Recovery room monitoring (2-4 hours)
- Pain management with IV medications
- Vital sign monitoring
- Neurological checks (moving legs/arms, sensation)
Days 1-2:
- Physical therapy begins (sitting, standing, walking with assistance)
- Transition from IV to oral pain medications
- Catheter removed (usually day 1-2)
- Drain removed if placed
- Ice therapy for swelling
- Hospital stay: 1-4 days depending on procedure
Discharge criteria:
- Adequate pain control with oral medications
- Able to walk independently or with walker
- No signs of infection or complications
- Can perform basic self-care
- Understanding of home instructions
Early Recovery: Weeks 1-6
Week 1:
- Pain: Moderate to severe, gradually improving
- Activity: Short walks (5-10 minutes) 3-4 times daily
- Restrictions: No bending, lifting >5 lbs, twisting
- Goals: Prevent complications, basic mobility
Common challenges:
- Muscle spasms
- Difficulty finding comfortable sleeping position
- Medication side effects (constipation, nausea)
- Dependency for household tasks
Weeks 2-3:
- Pain: Improving but still significant
- Activity: Gradually increase walking distance (15-20 minutes)
- May start: Gentle stretching, stationary cycling (if cleared)
- Follow-up: First post-op appointment around week 2
Weeks 4-6:
- Pain: Should be significantly better than pre-surgery
- Activity: Walking 30-45 minutes
- May resume: Light household activities, short car rides
- Physical therapy: May begin formal PT (if recommended)
- Return to work: Possible for sedentary jobs
Red flags requiring immediate medical attention:
- Fever >101.5°F
- Increasing redness, swelling, or drainage from incision
- New or worsening weakness
- Loss of bowel/bladder control
- Chest pain or difficulty breathing
- Severe headache (spinal fluid leak)
- Calf pain or swelling (blood clot)
Mid-Recovery: Weeks 6-12
Weeks 6-8:
- Pain: Mild to moderate, mostly with activity
- Activity: Progress to 1-hour walks
- May resume: Driving (if off narcotics), swimming
- Physical therapy: Core strengthening, flexibility work
- Return to work: Most sedentary workers back by 6-8 weeks
Weeks 8-12:
- Imaging: X-rays to assess fusion healing (for fusion patients)
- Activity: Gradually increase intensity
- May resume: Light resistance training, golf, non-impact sports
- Lifting: Up to 20-30 lbs if cleared
- Return to work: Light-duty physical workers
Goals for 3 months:
- Independent in all activities of daily living
- Pain improved 50-70% from pre-surgery
- Discontinued or minimal narcotic use
- Walking 1+ miles comfortably
- Basic core strength restored
Late Recovery: Months 3-6
Months 3-4:
- Bone fusion: 50-70% healed (for fusion patients)
- Activity: Progressive return to normal activities
- May resume: Jogging (if cleared), cycling, tennis
- Work: Most patients fully back to work
Months 4-6:
- Pain: Should be minimal
- Function: Near baseline or better
- Restrictions: Gradually lifted
- May resume: Most recreational activities
- Physical therapy: Often completed
Long-Term Recovery: 6-12+ Months
Months 6-12:
- Bone fusion: Complete by 12 months
- Activity: Full return to sports and physical activities
- Outcome assessment: Final evaluation of surgical success
Beyond 1 Year:
- Continued strength and flexibility improvement
- Maintenance exercise program essential
- Annual or as-needed follow-ups
- Monitoring for adjacent segment disease
Physical Therapy and Rehabilitation
1 (Weeks 1-6): Protection
- Focus: Prevent complications, gentle mobility
- Exercises: Walking, ankle pumps, deep breathing
- Avoid: Spinal flexion, rotation, lifting
2 (Weeks 6-12): Mobility
- Focus: Restore normal movement patterns
- Exercises: Stretching, aquatic therapy, stationary bike
- Progressively increase: Range of motion, endurance
3 (Months 3-6): Strengthening
- Focus: Core stability, functional strength
- Exercises: Resistance training, balance work, sport-specific training
- Goal: Return to desired activities
4 (6+ Months): Maintenance
- Focus: Prevent recurrence, optimize function
- Exercises: Continued strength and flexibility program
- Lifestyle: Weight management, posture awareness, activity modification
Home exercise compliance is the single best predictor of long-term success.
Preparing for Spinal Surgery
Proper preparation significantly improves outcomes and reduces complications.
Medical Evaluation and Clearance
Required tests:
- Blood work (CBC, metabolic panel, coagulation studies)
- EKG and chest X-ray (if over 50 or heart/lung disease)
- Cardiac clearance (for high-risk patients)
- Dental clearance (infection source)
Medication adjustments:
- Stop 7-14 days before: NSAIDs, blood thinners (except if directed otherwise)
- Stop 2 weeks before: Herbal supplements (can affect bleeding/anesthesia)
- Continue: Most blood pressure and heart medications
- Insulin adjustments: Your doctor will provide specific instructions
Pre-Surgical Optimization
Smoking cessation:
- Critical: Stop 4-8 weeks before surgery
- Reduces infection risk
- Dramatically improves fusion rates
- Consider nicotine replacement therapy
Weight loss:
- Even 5-10 lbs reduces complication risk
- May defer elective surgery if BMI >40
Nutrition:
- Protein intake: 1 gram per kg body weight
- Vitamin D optimization (levels >30 ng/mL)
- Multivitamin with minerals
Glucose control:
- HbA1c <7% preferred for diabetics
- May need endocrinology consultation
Home preparation:
- Install grab bars in bathroom
- Arrange sleeping on main floor
- Stock up on groceries
- Prepare frozen meals
- Arrange help for first 2-4 weeks
Psychological preparation:
- Set realistic expectations
- Develop coping strategies
- Line up support system
- Consider counseling if anxious/depressed
What to Expect on Surgery Day
Arrival (Usually 2 hours before surgery):
- Check-in and registration
- Change into surgical gown
- IV placement
- Anesthesia consultation
- Surgeon marks surgical site
Anesthesia:
- General anesthesia (you’ll be completely asleep)
- Intubation for breathing support
- Monitoring lines placed
Surgery duration:
- Varies by procedure: 1-6+ hours
- Discectomy: 1-2 hours
- Single-level fusion: 2-4 hours
- Multi-level fusion: 4-8+ hours
Intraoperative monitoring:
- Neurophysiological monitoring (tracks nerve function in real-time)
- Reduces nerve injury risk
- Surgeon alerted immediately to any changes
Recovery room:
- 2-4 hours after surgery
- Close monitoring as you wake up
- Family usually allowed brief visits
Life After Spinal Surgery: What to Expect
Understanding realistic long-term outcomes helps set appropriate expectations.
Pain Management Post-Surgery
Immediate post-op (Days 1-7):
- Opioid medications typically needed
- Muscle relaxants for spasms
- Nerve pain medications if needed
Weeks 2-6:
- Transition to non-opioid options
- NSAIDs (once cleared by surgeon)
- Acetaminophen
- Topical therapies
Months 3+:
- Most patients off pain medications
- Occasional OTC use for flare-ups
Important: Opioid weaning should be planned from the start to prevent dependency.
Pain patterns:
- Surgical site pain resolves over weeks
- Pre-existing nerve pain may take months to fully improve
- Some patients have different pain post-surgery
- 10-40% have persistent pain (failed back surgery syndrome)
Activity Restrictions
Typical restrictions after fusion surgery:
| Activity | Restriction Period |
| Lifting >5 lbs | 6-12 weeks |
| Bending at waist | 6-12 weeks |
| Twisting | 6-12 weeks |
| Driving | 2-6 weeks (off narcotics) |
| Sexual activity | 4-6 weeks |
| Swimming | 6-8 weeks |
| Golf | 3-6 months |
| Contact sports | 6-12 months |
| Heavy lifting (>50 lbs) | 6-12 months |
Note: Minimally invasive procedures often have shorter restriction periods.
Returning to Work
Sedentary jobs (desk work):
- 4-8 weeks typical
- May start part-time at 4-6 weeks
- Full-time by 8 weeks
Light-duty physical jobs:
- 8-12 weeks typical
- May need temporary restrictions
- Gradual return to full duties
Heavy labor (construction, nursing, firefighting):
- 3-6 months minimum
- May require permanent restrictions
- Some patients need career transition
Disability considerations:
- Short-term disability: Typically covers 6-12 weeks
- Long-term disability: May be needed if permanent restrictions
- Social Security Disability: For those unable to return to any work
Long-Term Lifestyle Modifications
Essential habits for spine health:
Exercise:
- Daily walking (30-60 minutes)
- Core strengthening 3x/week
- Flexibility/stretching program
- Low-impact aerobics (swimming, cycling)
Ergonomics:
- Proper workstation setup
- Lifting technique (knees, not back)
- Frequent position changes
- Lumbar support when sitting
Weight management:
- Each pound of excess weight = 4 lbs pressure on spine
- BMI <30 significantly reduces future problems
Smoking cessation:
- Continued smoking accelerates spine degeneration
- Increases adjacent segment disease risk
Stress management:
- Chronic stress worsens pain perception
- Mindfulness, meditation, or counseling
Success Rates and Realistic Outcomes
Leg/arm pain (radiculopathy):
- 85-95% significant improvement
- Often resolves completely
Back/neck pain:
- 60-80% moderate improvement
- Complete resolution rare
- Results more variable than with radiculopathy
Function:
- Most patients return to desired activities
- May need modifications for high-impact sports
- Work return rates: 70-85%
Patient satisfaction:
- 70-85% satisfied or very satisfied
- Higher satisfaction when expectations aligned with outcomes
- Second surgeries have lower satisfaction rates
Factors predicting success:
- Clear diagnosis matching symptoms
- Failed conservative treatment trial
- Positive attitude and motivation
- Strong support system
- Non-smoker
- Healthy weight
- Compliance with rehabilitation
Factors predicting poor outcomes:
- Psychological issues (depression, catastrophizing)
- Litigation/compensation claims
- Multiple prior surgeries
- Smoking
- Obesity
- Unrealistic expectations
- Diffuse, non-specific pain
Top 5 Spine Surgeons in Hyderabad, India
| Rank | Surgeon Name | Credentials | Specialization | Hospital Affiliation | Notable Achievements |
| 1 | Dr. Kiran Kumar Lingutla | MS (Ortho), MCh (Neuro), Fellowship (UK) | Complex spine surgery, minimally invasive spine surgery, spinal deformity correction | Yashoda Hospitals, Somajiguda | • International training in UK• Expertise in complex spinal reconstructions• Pioneer in minimally invasive techniques in Telangana |
| 2 | Dr. Ravi Suman Reddy | MS (Ortho), Fellowship Spine Surgery | Spinal deformity, minimally invasive spine surgery, disc replacement | KIMS Hospitals, Secunderabad | • Over 15,000 spine surgeries performed• Expert in artificial disc replacement• Specializes in scoliosis correction |
| 3 | Dr. Surya Prakash | MS (Ortho), DNB (Ortho), Fellowship Spine | Degenerative spine conditions, spinal trauma, endoscopic spine surgery | Sunshine Hospitals, Gachibowli | • Advanced endoscopic spine surgery• Expertise in geriatric spine surgery• Published researcher in spine journals |
| 4 | Dr. Sangam Rajesh | MCh (Neurosurgery), Fellowship Spine | Minimally invasive neurosurgery, complex spinal tumors, cervical spine surgery | Continental Hospitals, Gachibowli | • Expertise in spinal tumor resection• Advanced neuro-navigation techniques• International training in Germany |
| 5 | Dr. Phani Kiran S | MS (Ortho), DNB (Ortho), Fellowship (Germany) | Spinal deformity correction, revision spine surgery, pediatric spine | Care Hospitals, Banjara Hills | • Pediatric spine specialist• Expertise in revision complex cases• International faculty at spine conferences |
Top 5 Spine Surgeons in the World
| Rank | Surgeon Name | Country | Institution | Specialization | Notable Achievements |
| 1 | Dr. Richard Fessler | USA | Rush University Medical Center, Chicago | Minimally invasive spine surgery, spinal cord injury, complex spinal reconstructions | • Past President, Congress of Neurological Surgeons• Pioneer in minimally invasive techniques• Over 500+ peer-reviewed publications• Inventor of surgical instruments |
| 2 | Dr. Patrick Hsieh | USA | Keck Medicine of USC, Los Angeles | Complex spinal deformity, minimally invasive surgery, spinal oncology | • Director of Minimally Invasive Spine Surgery• International expert in adult deformity• Developed innovative surgical approaches• Trains surgeons worldwide |
| 3 | Prof. Juergen Harms | Germany | SRH Klinikum Karlsbad-Langensteinbach | Spinal deformity correction, scoliosis, kyphosis | • Developed the “Harms Technique” for C1-C2 fusion• Pioneer in 3-column osteotomy• Over 40 years of spine surgery experience• Trained hundreds of international surgeons |
| 4 | Dr. K. Daniel Riew | USA | Columbia University, New York | Cervical spine surgery, revision spine surgery, motion preservation | • World’s leading cervical spine surgeon• Expert in artificial disc replacement• Pioneered posterior cervical foraminotomy• Past President of Cervical Spine Research Society |
| 5 | Dr. Luiz Pimenta | Brazil | Instituto de Patologia da Coluna (IPC), São Paulo | Lateral lumbar interbody fusion, minimally invasive techniques | • Developed XLIF (eXtreme Lateral Interbody Fusion)• Over 20,000 minimally invasive procedures• International training center director• Published 200+ scientific papers |
Honorable Mentions – World Leaders
| Surgeon Name | Country | Institution | Key Expertise |
| Dr. Christopher Shaffrey | USA | Duke University | Complex spinal deformity, spinal oncology |
| Dr. Frank Kandziora | Germany | Center for Spine Surgery, Frankfurt | Cervical spine trauma, degenerative conditions |
| Prof. Max Aebi | Switzerland | University of Bern (Retired) | Spinal instrumentation pioneer, international educator |
| Dr. Alexander Vaccaro | USA | Rothman Orthopaedic Institute | Spinal trauma, thoracolumbar surgery |
| Dr. Praveen Mummaneni | USA | UCSF Medical Center | Complex spine, skull base surgery |
Frequently Asked Questions About Spinal Surgery
- How long does it take to fully recover from spinal surgery?
Full recovery varies significantly by procedure type. Minimally invasive discectomy patients often return to normal activities within 6-12 weeks, while spinal fusion requires 3-6 months for initial recovery and up to 12 months for complete bone fusion. Heavy laborers may need 6-12 months before returning to unrestricted work. Factors affecting recovery include age, overall health, smoking status, adherence to physical therapy, and whether complications occur. Most patients see their maximum improvement by the 1-year mark.
- What is the success rate of spinal surgery?
Success rates depend on the specific condition and procedure. For herniated discs causing leg pain, microdiscectomy has an 85-95% success rate for significant pain relief. Laminectomy for spinal stenosis provides 80-90% improvement in leg symptoms. Spinal fusion success is more variable—60-80% of patients report moderate to significant improvement in back pain. However, complete pain elimination is rare, and 10-40% experience failed back surgery syndrome. Success is highest when surgery addresses nerve compression rather than non-specific back pain, and when patients are carefully selected with realistic expectations.
- What are the most common complications from spinal surgery?
The most common complications include infection (1-3%), excessive bleeding requiring transfusion (1-5%), blood clots in legs (1-3%), and spinal fluid leak (1-3%). Nerve injury occurs in less than 1% of cases but can cause weakness or numbness. Failed back surgery syndrome—persistent or worsening pain after surgery—affects 10-40% of patients and is technically a poor outcome rather than a complication. Hardware-related issues (screw loosening, rod breakage) occur in 2-5% of instrumented fusions. Smoking, diabetes, obesity, and revision surgery significantly increase complication risks.
Conclusion
Spinal surgery is generally considered for severe, persistent pain or neurological deficits (numbness, weakness) when non-surgical treatments fail, or in cases of instability, trauma, or structural deformity. Common procedures include discectomy, laminectomy, and fusion to relieve compressed nerves. While generally safe, risks include infection, nerve damage, and failed back surgery syndrome. Recovery typically involves immediate mobilization, with a return to light activity in 2–6 weeks and full recovery in 3–12 months.