


Food hypersensitivity affects millions worldwide, causing uncomfortable or even dangerous reactions to everyday foods. It differs from simple preferences, demanding careful management to avoid symptoms like bloating or severe allergic responses.
Understanding it starts with knowing your body’s response to certain foods. This guide covers everything from basics to practical tips.
Table of Contents
What is Food Hypersensitivity?
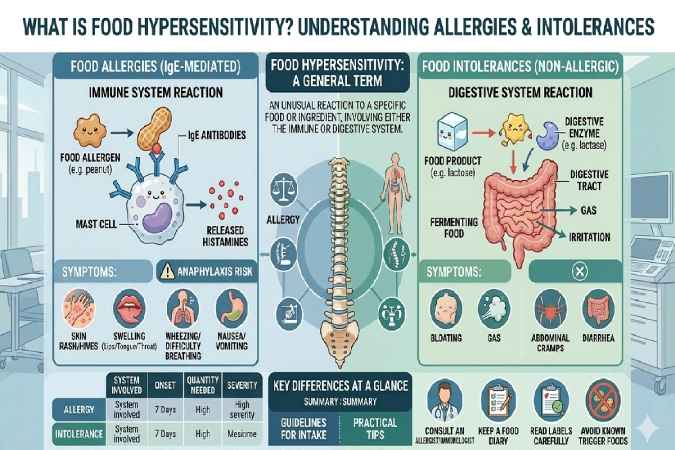
Food hypersensitivity describes any adverse reaction to food, ranging from immune-driven allergies to digestive intolerances. Unlike a true allergy, which involves the immune system attacking harmless proteins, hypersensitivity casts a wider net including non-immune issues.
Types of Food Hypersensitivity
Healthcare experts define food hypersensitivity as an abnormal response to food components, often proteins or enzymes. It splits into IgE-mediated (quick, severe like hives or anaphylaxis) and non-IgE (delayed, like chronic gut issues). Intolerances, such as lactose issues, fall under non-immune hypersensitivity due to enzyme shortages.
For example, eating ice cream might trigger immediate swelling in an IgE case but hours-later cramps in intolerance.
Food Hypersensitivity vs. Food Allergy vs. Intolerance
| Aspect | Food Hypersensitivity | Food Allergy | Food Intolerance |
| Mechanism | Immune or non-immune | IgE immune-mediated | Non-immune (e.g., enzyme lack) |
| Onset | Minutes to hours/days | Minutes | Hours to days |
| Symptoms | GI, skin, respiratory | Anaphylaxis possible | Bloating, gas, no life-threat |
| Test | Varies (skin/blood/challenge) | IgE tests | Elimination diet |
Allergies pose anaphylaxis risk, needing epinephrine; intolerances allow small amounts sometimes.
Common Symptoms of Food Hypersensitivity
Reactions vary but often hit gut, skin, or airways. Track patterns after meals for clues.
Gastrointestinal Signs
Bloating, diarrhea, constipation, reflux, or vomiting top the list. Non-IgE types mimic IBS with ongoing discomfort.
Skin and Respiratory Reactions
Rashes, eczema, hives, or wheezing occur, especially IgE-mediated. Oral itching signals issues.
When Symptoms Signal Emergency
Swelling, breathing trouble, or drop in blood pressure demand immediate care – carry epinephrine if history suggests allergy.
Causes and Risk Factors
Proteins in foods trigger immune overreactions or digestive glitches. Genetics play a role.
Immune-Mediated Mechanisms (IgE and Non-IgE)
IgE binds allergens fast; non-IgE involves cells like eosinophils, causing esophagitis.
Non-Immune Triggers
Lactose intolerance from lactase lack; FODMAPs in wheat/fruits ferment in gut.
Genetic and Environmental Influences
Family history raises risk; early antibiotics or hygiene hypothesis link to modern rises.
Prevalence hits 2-35% in kids, lower in adults; India sees dairy/gluten spikes.
Common Trigger Foods
Milk, eggs, nuts, gluten, seafood lead globally.
Top Allergens Worldwide and in India
| Food | Prevalence Notes | Hidden In |
| Cow’s milk | 33% cases | Breads, chocolates |
| Gluten/wheat | 57% | Sauces, processed foods |
| Nuts/peanuts | 27-20% | Snacks, oils |
| Eggs | 20% | Baked goods, mayo |
| Spices (India) | Regional, cumin/chili | Curries, masalas |
Treatment Of Food Hypersensitivity
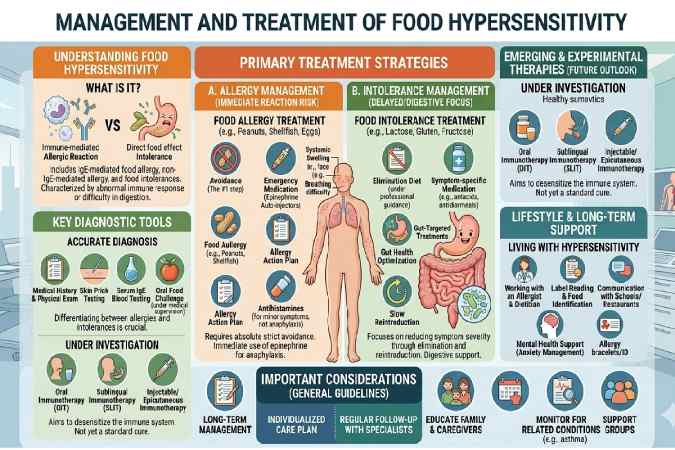
Treating food hypersensitivity focuses on avoiding triggers while managing symptoms effectively. Options range from strict diets to advanced therapies, tailored to whether it’s immune-mediated or non-immune.
Primary Treatment: Avoidance
The cornerstone is eliminating trigger foods after proper diagnosis. This prevents reactions but requires careful planning to avoid nutritional gaps, especially in vegetarian diets common in India.
Work with a dietitian for elimination diets: Remove suspects for 4-6 weeks, then reintroduce one by one under supervision. For intolerances like lactose, enzyme supplements (e.g., lactase pills) allow limited intake.
Acute Reaction Management
For IgE-mediated hypersensitivity mimicking allergies:
- Epinephrine autoinjectors (e.g., EpiPen) for anaphylaxis – inject immediately into thigh if swelling, breathing issues, or drop in blood pressure occur.
- Follow with antihistamines (e.g., cetirizine) for hives/itching and corticosteroids if needed.
| Reaction Severity | Immediate Steps | Follow-Up Care |
| Mild (rash, nausea) | Antihistamine; rest | Monitor 4-6 hours |
| Moderate (vomiting, swelling) | Antihistamine + call doctor | Oral steroids if persistent |
| Severe (anaphylaxis) | Epinephrine; ER | 2-dose prescription; allergist referral |
Carry two doses always; train family/schools.
Long-Term Therapies
- Medications: Antihistamines or proton pump inhibitors (PPIs) for gut symptoms like reflux in non-IgE cases. Biologics like omalizumab (Xolair) reduce reaction risks for confirmed allergies.
- Immunotherapy:
- Oral immunotherapy (OIT): Gradual daily doses of allergen (e.g., peanut powder like Palforzia) build tolerance. Effective for milk/egg/peanut in kids; 67-95% desensitize but needs monitoring for side effects.
- Sublingual immunotherapy (SLIT): Drops under tongue; safer for home use, good for peanut.
- Emerging: Multi-food OIT for 30% with multiple triggers.
Not cures – maintenance doses often lifelong. Available via allergists; research advances in 2025+ trials.
Nutritional and Lifestyle Support
Balance diets to prevent deficiencies:
- Dairy-free? Fortified plant milks, ragi, sesame for calcium.
- Gluten-free? Millets (jowar, bajra), rice-based Indian meals.
- Monitor growth in kids via regular check-ups.
| Nutrient | Alternatives for Hypersensitivity Diets |
| Calcium | Leafy greens, almonds (if tolerated), fortified soy |
| Protein | Lentils, quinoa, eggs (if non-egg trigger) |
| B12/Iron | Supplements if vegan avoidance heavy |
Emerging and Preventive Options
- Probiotics/gene therapy: Early research for gut modulation; not standard yet.
- Prevention: Introduce allergens early (4-6 months) in infants to cut risk.
Consult allergists for personalized plans – missteps risk malnutrition or reactions. In India, urban centers offer OIT; track via apps for symptoms.
Top 20 Food Allergies
The top food allergies worldwide are primarily the “Big 9” (or “Big 8” before sesame’s addition), accounting for over 90% of reactions, with others varying by region like Asia or India. Rankings are based on prevalence data from sources like FARE, Mayo Clinic, and global studies, prioritizing IgE-mediated cases in children and adults.
Here’s a ranked list of the top 20, drawing from epidemiological surveys (e.g., US/Europe highest for nuts/milk; Asia for shellfish/sesame). Prevalence decreases down the list; exact % varies (e.g., peanuts ~1-2% kids globally).
| Rank | Food Allergen | Key Notes & Prevalence Highlights |
| 1 | Cow’s milk | Most common in infants (2-3%); 90% outgrow by age 3; hidden in formulas/baked goods. |
| 2 | Eggs | Affects ~2% young children; often outgrown; in vaccines/baked items. |
| 3 | Peanuts | ~1-2% kids (higher in West); persistent into adulthood; severe anaphylaxis risk. |
| 4 | Tree nuts (e.g., almonds, walnuts) | ~1% prevalence; 40% cross-react with peanuts; lifelong for many. |
| 5 | Soy | 0.4% kids; common in Asia; often outgrown; in tofu/edamame/processed foods. |
| 6 | Wheat | ~0.5-1%; celiac overlap; gluten proteins trigger; global staple issue. |
| 7 | Shellfish (e.g., shrimp, crab) | Top adult allergen (~2%); prevalent in Asia; lifelong, potent reactions. |
| 8 | Fish (e.g., salmon, tuna) | ~0.5-1% adults; common in coastal areas; heat-stable allergens. |
| 9 | Sesame | Emerging (9th major US allergen 2021); up to 17% co-allergic with nuts; in tahini/breads. |
| 10 | Mustard | Common in Europe/India; seeds/spices; often overlooked in sauces. |
| 11 | Celery | Frequent in Europe; cross-reacts with birch pollen; in soups/stocks. |
| 12 | Lupin | Rising in Europe (legume like soy); in flours/baked goods. |
| 13 | Buckwheat | Asia/Japan staple allergy; in soba noodles. |
| 14 | Fruits (e.g., peach, kiwi) | Oral allergy syndrome; pollen cross-reactivity; raw fruit triggers. |
| 15 | Avocado | Latex-fruit syndrome link; in guac/cosmetics. |
| 16 | Banana | Cross-reacts with latex/pollen; tropical regions. |
| 17 | Garlic | Rare but rising; in savory dishes worldwide. |
| 18 | Chickpea (e.g., hummus) | India/Middle East; legume family. |
| 19 | Corn | Underreported; in sweeteners/processed foods. |
| 20 | Rice | Rare globally but noted in Asia; hydrolyzed proteins. |
Regional notes: In India (your location), prioritize milk, eggs, nuts, seafood, and spices like mustard/chickpea due to dietary habits. Always verify via allergy testing, as self-reports overestimate.
FAQ SECTION
What is the difference between food hypersensitivity and food allergy?
Food hypersensitivity includes both immune (allergy) and non-immune reactions; allergy specifically means IgE-mediated with potential anaphylaxis.
What are common symptoms of food hypersensitivity?
Symptoms include bloating, diarrhea, rashes, hives, reflux, or wheezing, varying by type.
How do you test for food hypersensitivity?
Use skin prick tests, blood IgE, elimination diets, or oral food challenges under medical supervision.
What foods most commonly cause food hypersensitivity?
Cow’s milk, gluten, eggs, nuts, wheat, and seafood top lists; spices in India.
Can food hypersensitivity go away?
Some kids outgrow IgE allergies; intolerances managed lifelong but symptoms lessen with enzymes/diets.
Is food hypersensitivity the same as lactose intolerance?
No – lactose is non-immune intolerance; hypersensitivity broader, often immune.
How to manage food hypersensitivity on a vegetarian Indian diet?
Use lactose-free paneer alternatives, gluten-free millets, nut-free proteins like lentils; consult dietitians.
Conclusion
Food hypersensitivity requires personalized avoidance, symptom management, and professional guidance to live symptom-free. Early diagnosis and balanced nutrition prevent complications, with therapies like OIT offering hope for tolerance.